Specialists
Years of experience in genetics, laboratory diagnostics and bioinformatics
Search for deletions and duplications in the dystrophin gene
Clinical characteristics
Dystrophinopathies are a group of X-linked neuromuscular diseases, both mild and severe, whose development is caused by mutations in the DMD geneencoding the distorphin protein.
The severity of the disease is determined by the type of mutation and the functional domainin which it is localized.
Mild course
Characterized by asymptomatic elevation of serum creatine phosphokinase and muscle convulsions with myoglobinuria.
Severe course
Manifested by the development of classic syndromes that include progressive Duchenne muscular dystrophy (PDMD), progressive Becker muscular dystrophy (PBMD) and DMD gene-associated dilated cardiomyopathy.
The disease is characterized by progressive weakness of the proximal muscles caused by degeneration of the muscle fibers. Degeneration occurs as a result of impaired stability and elasticity of muscle fibers during contraction. As the disease progresses, the muscle fiber is almost completely destroyed and replaced by connective tissue, resulting in muscle pseudohypertrophy — an increase in muscle volume with a loss or significant weakening of functionality. DMD is included in the list of the most common X-linked diseases [1].
Progressive muscular dystrophy usually begins with increased fatigue and weakness in the muscles of the lower extremities.
Differential diagnosis
Dystrophin

Dystrophin is a membrane protein, and the dystrophin-associated complex is the most important element of the muscle cytoskeleton, which ensures the interaction of internal and external cell structures, participates in the regulation of calcium levels in the muscle and impulse transmission across the muscle fiber membrane.
Dystrophin is mainly found in muscle cells and some neurons. Normally, its function is to provide elasticity and stability of muscle fiber during contraction.
In the absence of dystrophin, the cell membrane is destroyed and, as a consequence, the muscle fiber is destroyed and replaced by connective tissue, which leads to a significant weakening of functionality.
79%of the total number of mutations are large deletions and duplications.
21%21% are small changes involving single-nucleotide substitutions, small insertions and deletions, and splice site mutations, with missense variants not characteristic of PDMD/PBMD [3].
Peculiarities of clinical manifestations are associated with the type of mutation in the dystrophin gene:
In PDMD
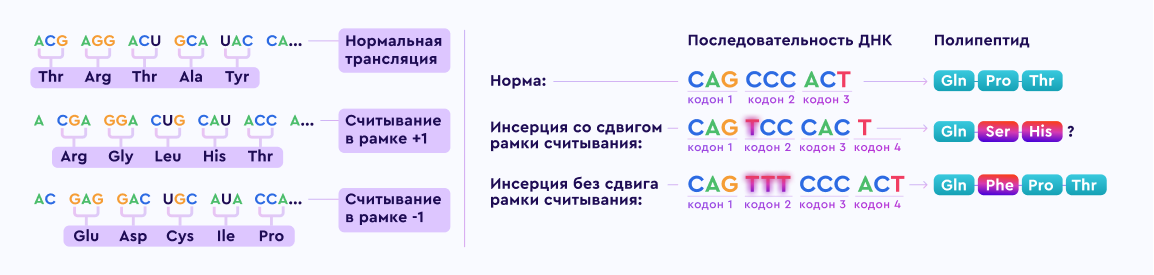
Deletions in the gene in most cases result in a frameshift and premature termination of the protein-building information, resulting in dystrophin not being formed.
In PBMD
Structural abnormalities in the gene do not disrupt the reading frame; as a result, a defective, functionally deficient protein is formed.
In DMD gene-associated dilated cardiomyopathy
Functionally active dystrophin is absent in the myocardium but is present in skeletal muscle, because in this type of dystrophinopathies pathogenic variants result in different tissue-specific transcription or alternative splicing in cardiac muscle and in skeletal muscle [Ferlini et al 1999, Neri et al 2007].
Progressive Duchenne muscular dystrophy
This is the more common form of the disease. The first signs appear at an early age (1-5 years) and are characterized by delayed motor development. At the beginning of walking, frequent falls, awkwardness and fatigue, difficulties in climbing stairs, running and jumping are noted. Patients retain the ability to walk until the age of 10-12 years. Cardiomyopathy develops in almost all patients with PDMD after the age of 18.
The disease progresses rapidly and death usually occurs before the age of 30 as a result of respiratory complications and progression of dilated cardiomyopathy.
Progressive Becker muscular dystrophy
Generally characterized by later manifestation and milder clinical signs. Clinical signs begin to manifest around the age of 10 to 20 years. The disease progresses quite slowly, in most cases, the patient loses the ability to move without a wheelchair no earlier than the age of 40.
Despite the milder neuromuscular phenotype, heart failure is the most frequent cause of death in PBMD (the average age of death is 40-50 years).
DMD gene-associated dilated cardiomyopathy
According to sources, mutations in the DMD gene can cause not only DMD/BMD but also dilated cardiomyopathy 3B [2,6], which is a disease of the heart muscle that leads to ventricular dysfunction and, consequently, heart failure. Women heterozygous for the pathogenic variant are at high risk of developing this pathology.
1:5000newborn boys
Progressive Duchenne muscular dystrophy [4]
1:20-25000
Progressive Becker muscular dystrophy [9]
Xp21.2–p21.1The dystrophin gene is localized on the short arm of the X chromosome (Xp21.2-p21.1) and is one of the longest in the human genome (over 2Mb, containing 79 exons).
Dystrophinopathies are X-linked recessive diseases by type of inheritance. The penetrance of dystrophinopathies is complete in hemizygous boys; it varies in heterozygous girls carrying the pathogenic variant.
If a woman is a carrier of a heterozygous pathogenic mutation in the DMD gene, the probability of transmission of the mutation:

If pregnant with a boy — 50%The mutation will be passed on to the son and he will have PDMD/PBMD.
All boys who inherit the pathogenic variant from their mother will be sick.
If pregnant with a girl — 50%The daughter will inherit this mutation and will be a carrier of the defective copy of the DMD gene.
Girls who inherit the pathogenic variant may be asymptomatic carriers of the pathogenic mutation in a heterozygous state or may have clinical manifestations of classical dystrophinopathy.
Conditions of occurrence
At the same time, identification of heterozygous female carriers is important for clinical monitoring of cardiac pathologies in such patients.
Male PDMD patients usually do not manage to leave offspring because of early death; patients with PBMD and DMD gene-associated dilated cardiomyopathy can have offspring: all their daughters will be heterozygous carriers of the pathogenic variant and none of their sons will inherit the pathogenic variant.
Detection of carriage of the DMD gene DMD gene mutation and family planning for the risk of having a sick child is the most effective way to prevent dystrophinopathies.
The father of a sick boy usually does not need molecular genetic testing because if he is healthy, he cannot be hemizygous for the pathogenic variant.
The residual risk is the probability of giving birth to a boy with dystrophinopathy even if the maternal DMD gene testing does not show carriage of the pathogenic variant in the leukocyte DNA.
The existence of a residual risk is due to the fact that in 15-20% of cases, the development of muscular dystrophy is due to a de novo mutation (gonadal mosaicism is most likely) [5]. In such a case, all the siblings of a male proband also have an increased risk of inheriting the pathogenic variant and prenatal diagnosis in subsequent pregnancies is advisable.
Progressive Duchenne muscular dystrophy:
Progressive Becker muscular dystrophy:
DMD gene-associated dilated cardiomyopathy
Methods of molecular genetic diagnosis
The approach to molecular genetic diagnosis of dystrophinopathies consists of the following steps in sequence:
1. Тest DMD gene
Since most pathogenic variants are deletions/duplications of one or more exons, it is advisable to start with copy number variation analysis (MLPA, chromosomal exon microarray analysis). If no pathogenic variant is detected, the next step is to sequence the DMD gene (given the length of the gene, it is possible to start the search from "hotspots").
2. Studying a panel of genes
Search for mutations that are characteristic of neuromuscular diseases, including those with similar clinical manifestations (read "Differential Diagnosis").
3. Advanced genetic testing
Full-exome or full-genome sequencing can be performed in cases of atypical clinical manifestations, in order to refine the diagnosis and identify possible causal findings in other genes.
The test is usually performed based on information about previously identified pathogenic variants in the DMD gene in family members.
Biological samples suitable for molecular genetic testing:
Literature Cited:
1. Marina Basta, Ashish M. Pandya. Genetics, X-Linked Inheritance. Treasure Island. 2021 Jan; PMID: 32491315
2. https://www.omim.org/entry/302045
3. Hum Mutat. The TREAT-NMD DMD Global Database: Analysis of More than 7,000 Duchenne Muscular Dystrophy Mutations. Human Mutation. 2015 Apr; 36(4): 395–402.
4. Eppie M Yiu, Andrew J Kornberg. Duchenne muscular dystrophy. J Paediatr Child Health 2015 Aug; 51(8):759-64
5. "A method for molecular genetic testing for carriage of deletions and duplications of exons of the DMD gene. Authors: Vilchuk K.U., Gusina N.B., Gusina A.A., Myasnikov S.O., 2016.
6. Nakamura A. X-Linked Dilated Cardiomyopathy: A Cardiospecific Phenotype of Dystrophinopathy. Pharmaceuticals (Basel) 2015; 8:303–320.
7. Maria Sofia Falzarano, Chiara Scotton, Chiara Passarelli, Alessandra Ferlini. Duchenne Muscular Dystrophy: From Diagnosis to Therapy. Molecules. 2015 Oct 7; 20(10):18168-84.
8. Van Westering T.L.E., Betts C.A., Wood M.J.A. Current understanding of molecular pathology and treatment of cardiomyopathy in Duchenne Muscular Dystrophy. Molecules. 2015
9. Ivanov V.I., Baryshnikova N.V., Bileva D.S., Dadali E.L., Genetics. 2006

Years of experience in genetics, laboratory diagnostics and bioinformatics

All data is strictly confidential and cannot be passed on to third parties

Extensive control at each stage of testing

Results ready in a short time

Free delivery of biomaterial across Russia
— presence of a deletion of the X chromosome in the Xp21.2 region;
— single parental dysomy on the X chromosome;
— compound heterozygous state of two pathogenic variants;
— non-random X-inactivation
Номер 8 (800) 201–83–46
не работает по техническим причинам
Или пишите на info@f-genetics.com — обязательно вам ответим