The dystrophin gene is localized on the short arm of the X chromosome (Xp21.2-p21.1) and is one of the longest in the human genome. Dystrophinopathies are X-linked recessive diseases by type of inheritance.
Most cases are due to heterozygous maternal carriage of the abnormal mutation in the DMD gene.
If pregnant with a boy — 50%The mutation will be passed on to the son and he will have PDMD/PBMD.
All boys who inherit the pathogenic variant from their mother will be sick.
If pregnant with a girl — 50%The daughter will inherit this mutation and will be a carrier of the defective copy of the DMD gene.
Girls who inherit the pathogenic variant may be asymptomatic carriers of the pathogenic mutation in a heterozygous state or may have clinical manifestations of classical dystrophinopathy.
Detection of carriage of the DMD gene mutation and family planning for the risk of having a sick child is the most effective way to prevent dystrophinopathies.
The father of a sick boy usually does not need molecular genetic testing because if he is healthy, he cannot be hemizygous for the pathogenic variant.
The residual risk is the probability of giving birth to a boy with dystrophinopathy even if the maternal DMD gene testing does not show carriage of the pathogenic variant in the leukocyte DNA.
The existence of a residual risk is due to the fact that in 15-20% of cases, the development of muscular dystrophy is due to a de novo mutation (gonadal mosaicism is most likely) [5].
In such a case, all the siblings of a male proband also have an increased risk of inheriting the pathogenic variant and prenatal diagnosis in subsequent pregnancies is advisable.
Progressive Duchenne muscular dystrophy:
- The first signs appear before the age of 5.
- Low activity of the child is noted.
- Progressive symmetrical muscle weakness in the proximal parts.
- Frequent falls, motor clumsiness, rapid fatigue.
- Pseudohypertrophy of muscles (increased volume with decreased functionality), most frequently calf muscles, can manifest itself in the form of a false impression of an athletic physique.
- The pathological process has an ascending tendency. The muscles of the lower extremities are the first to be affected, then the shoulder girdle, back, and proximal parts of the upper extremities.
- At the early stages tendon reflexes are reduced.
- Around the age of 18, cardiomyopathy develops [8], which manifests as left ventricular hypertrophy and arrhythmia.
- Wheelchair dependence develops until the age of 13.
Progressive Becker muscular dystrophy:
- Debuts between the ages of 10 and 20 with the appearance of weakness and fatigue in the pelvic girdle and leg muscles.
- Muscle spasms become the early symptoms.
- The clinical manifestations are similar to PDMD, but milder.
- Progressive symmetrical muscle weakness in the proximal parts; weakness of the quadriceps femoris muscle is sometimes the only sign of the developing disease.
- Wheelchair dependence develops after age 16, although some patients retain independent motor activity in their 30s and rarely in their 40s.
- Hypogenitalism and testicular atrophy are detected in some cases [9].
Methods of molecular genetic diagnosis
The approach to molecular genetic diagnosis of dystrophinopathies consists of the following steps in sequence:
1. the DMD gene test DMD gene
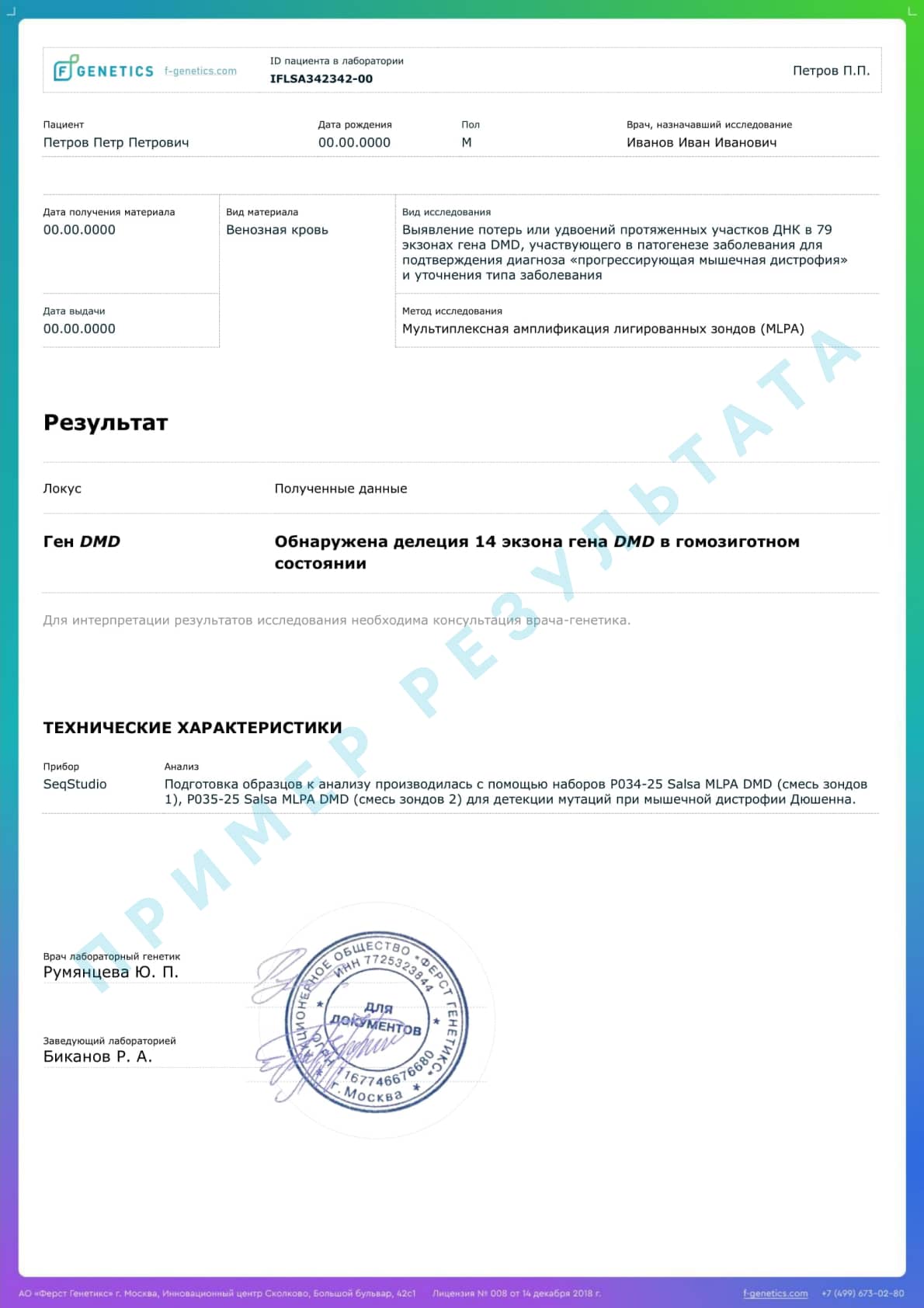
Since most cases of PDMD/PBMD are caused by the loss or doubling of long stretches of DNA, it is advisable to start by searching for mutations by MLPA (chromosomal exon microarray analysis).
If no pathogenic variant is detected, the next step is to sequence the DMD gene.
2. Studying a panel of genes
Mutations of which are characteristic of neuromuscular diseases, including those with similar clinical manifestations.
3. Advanced genetic testing
Including full-exome or full-genome sequencing can be performed in cases of atypical clinical manifestations, in order to clarify the diagnosis and establish possible causal findings in other genes.
The test is usually performed based on information about previously identified pathogenic variants in the DMD gene in family members.
Biological samples suitable for molecular genetic testing:
- Peripheral blood (EDTA tube)
- Amniotic fluid from 16 weeks of pregnancy
- Chorionic villi
- Umbilical cord blood (EDTA tube)